The Lower Eye Lift — and Why the Lift Comes From Above

Lower Eye LIft Blog
When patients come to us hoping to soften the under-eye, they usually point to three things at once: a hollow tear trough, puffy bags, and a cheek that no longer sits where it once did. These read as a single problem in the mirror. Surgically, they are three — and treating them well depends less on the incision than on how the tissue is supported afterwards.
A lower eye lift addresses the herniated orbital fat, repositions the descended midface, and re-drapes the under-eye. Done thoughtfully, it restores a rested look. Done with the wrong vector, it pulls the lid down. Here is how the procedure is actually built — and how an endoscopic temporal lift protects against its most feared complication.
What the Lower Eye Lift Addresses
Three changes converge under the eye. Herniated orbital fat creates the bag — fat that has pushed forward past a weakened retaining barrier. The tear-trough hollow appears as the cheek fat descends and the boundary between lid and cheek becomes a visible shadow. And the midface itself drops, lengthening the lower lid and flattening the cheekbone.
The elegant move in modern technique is to stop removing tissue and start repositioning it: the fat that bulges below is released and laid into the hollow above, so the bag fills the trough instead of being cut away. That single idea is why the dissection plane matters so much.
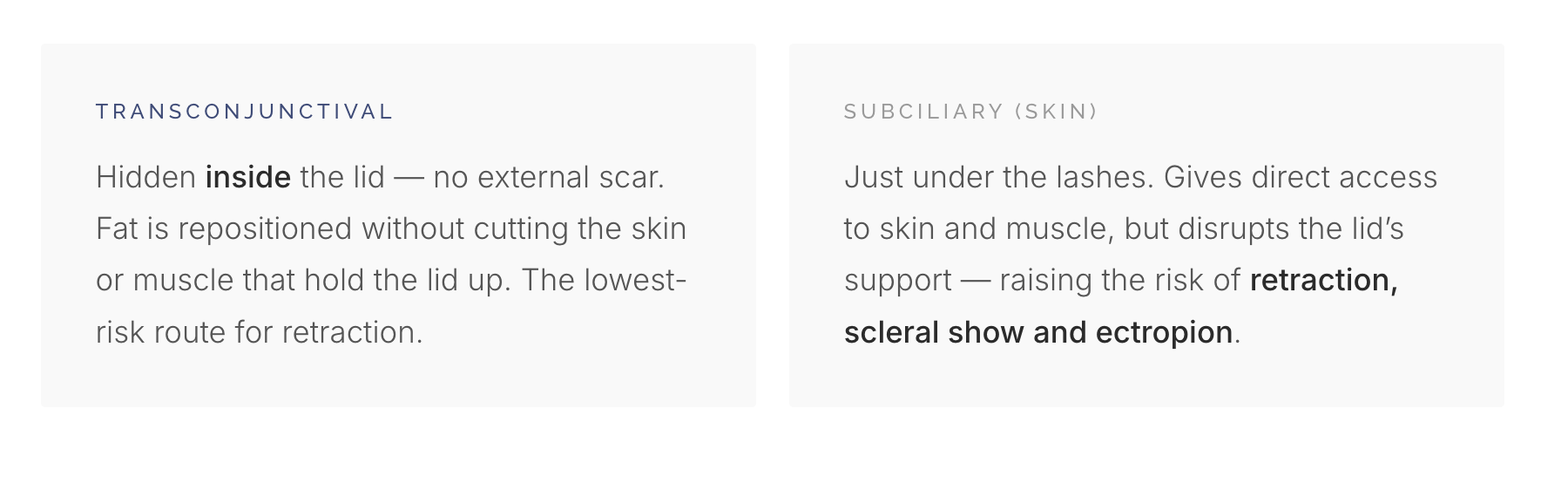
Two Ways In
Choosing the Access Route
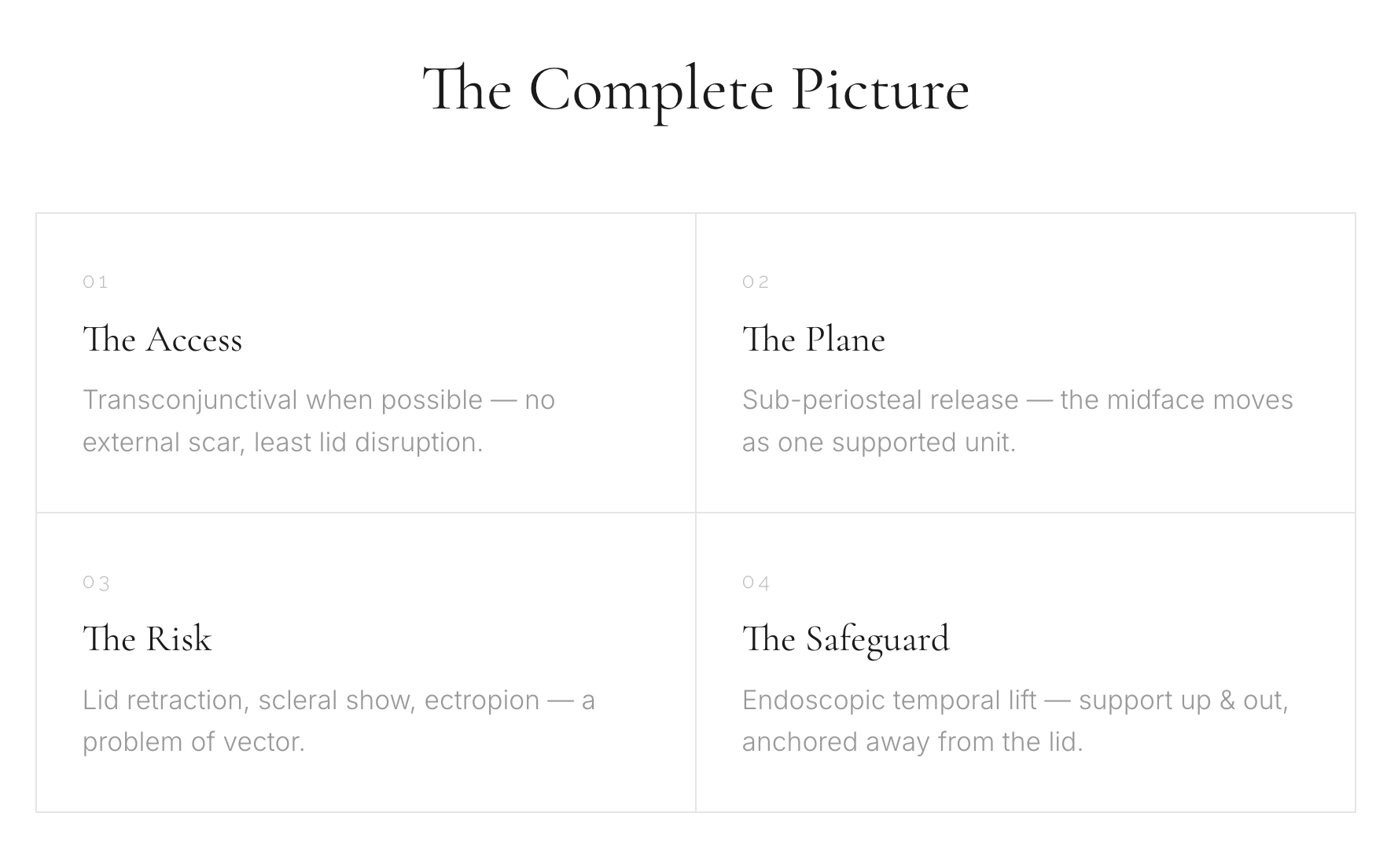
Everything begins with where the surgeon enters. The two routes differ not in what they can reach, but in how much they disturb the lower lid’s own support — which is exactly what determines the risk.
How the Dissection Plane Is Formed
To lift the midface as one stable unit, the surgeon develops a plane down over the cheekbone — most commonly the sub-periosteal plane, lifting fat, muscle and soft tissue up off the bone as a single composite rather than peeling it apart in layers.
Because the whole composite is freed and then re-suspended upward, the cheek fat that fell can be carried back up to refill the tear trough and support the lid from below — instead of thinning the lid itself. A clean, fully released plane is what lets the tissue move as one piece and hold its new position over time.
“The danger is rarely the incision alone.
It’s where the support comes from.”
The Risk
When the Lid Is Pulled Down
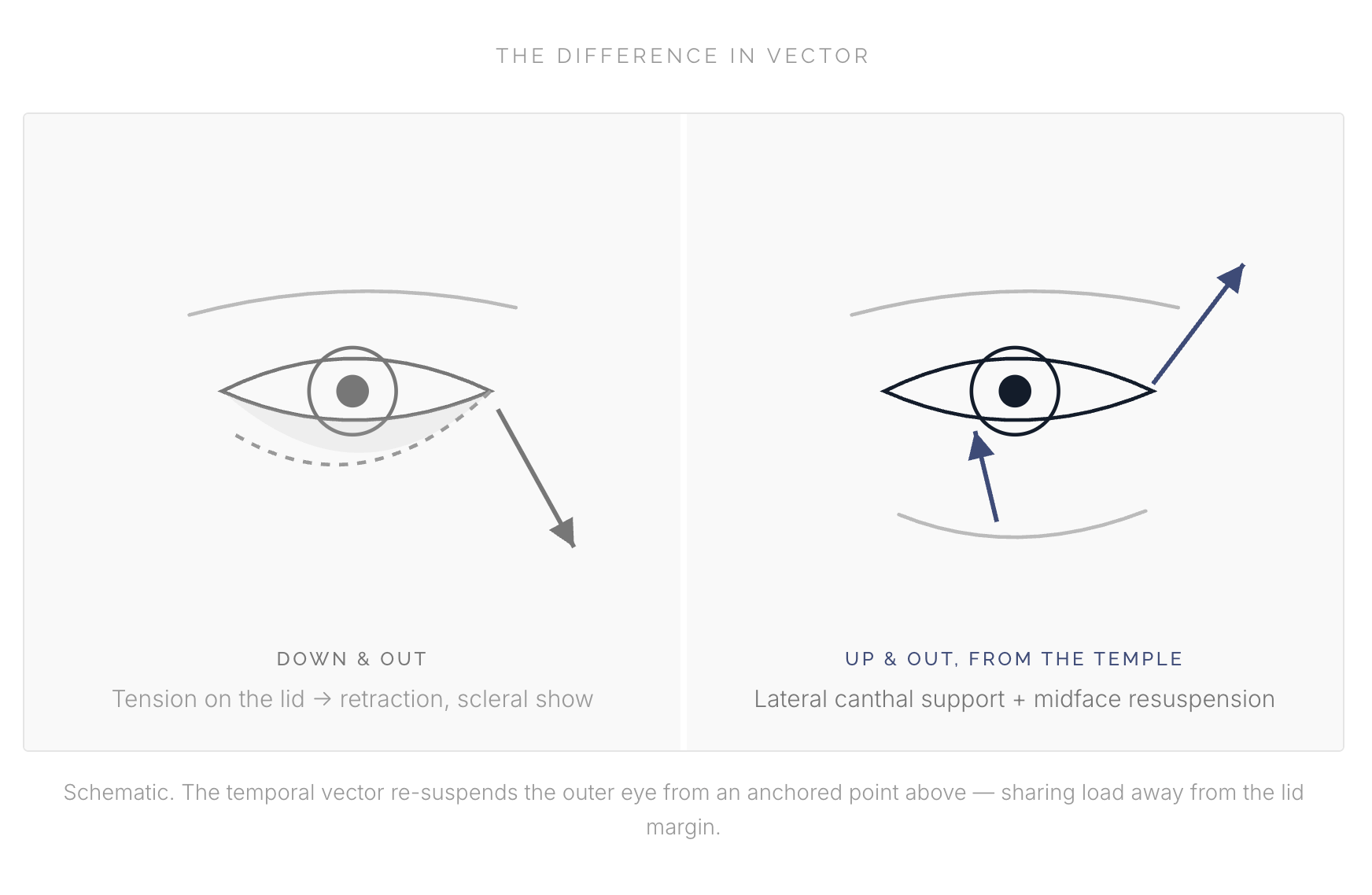
The feared outcome of any lower-lid work is the lid drifting down and out. When the lower lid loses its lateral support — whether from a skin incision’s scar contracture, gravity on freshly released tissue, or tension loaded onto the fragile lid margin — the result is retraction, scleral show (white showing beneath the iris), and in the worst case ectropion, where the lid turns outward.
It is the single signature of an over-pulled lower eye. And it is almost always a problem of vector — of lifting in the wrong direction, from the wrong anchor.
How the Endoscopic Temporal Lift Prevents It
An endoscopic temporal lift works through small incisions hidden in the hairline at the temple. Rather than relying on the lid itself, it lifts the lateral brow and the lateral orbicularis–canthal complex upward and outward — re-suspending the outer corner of the eye from above and to the side.
The lifting force is anchored at a strong point in the temple and shared across the whole lateral complex, instead of dragging on the lid edge. The lid is held up, not pulled down.

So Where Does the Lift Come From?
From above, and from the side — never from the lid itself. The lower eye lift restores the fat, the trough and the midface; the endoscopic temporal lift gives that work a strong, anchored point to hang from. Together they refresh the under-eye without the tell-tale signs of an over-pulled result.
At Surgery and Beyond, we coordinate this kind of considered, layered plan with Thailand’s most experienced specialists — so you return home looking naturally, beautifully refreshed.